OSUmetstud
-
Posts
16,521 -
Joined
-
Last visited
Content Type
Profiles
Blogs
Forums
American Weather
Media Demo
Store
Gallery
Everything posted by OSUmetstud
-
Major LES event-December 24-27
OSUmetstud replied to BuffaloWeather's topic in Upstate New York/Pennsylvania
I think Saturday morning is the best chance for good LES in BUF now as some warm advection kicks on the tail end of the trough. At least with the synoptic low trending east, you end up getting more snow for Christmas morning. -
Major LES event-December 24-27
OSUmetstud replied to BuffaloWeather's topic in Upstate New York/Pennsylvania
I think the band starts Friday morning regardless of model qpf outputs. It's a bit sheared then for sure, but good enough for a moderate band of lake effect over the southern side of BUF. It gets better later in the day due to increased instability and less shear. -
Major LES event-December 24-27
OSUmetstud replied to BuffaloWeather's topic in Upstate New York/Pennsylvania
It doesnt look like a big lightning producer to me, maybe an odd strike or two. The inversion is close to 700mb which is fine for heavy snow in a cold airmass, but its not great for lightning as the -10c isotherm is so close to the ground. -
Major LES event-December 24-27
OSUmetstud replied to BuffaloWeather's topic in Upstate New York/Pennsylvania
The westward trends with the synoptic low are better for BUF, it increases the duration of southwesterlies on the backside. -
Pretty good.
-
Mesos seemed better with this one in general.
-
Brutal
-
That's great. The early animal studies weren't clear that these vaccines were going to reduce transmission.
-
Active mid December with multiple event potential
OSUmetstud replied to Typhoon Tip's topic in New England
Yeah...I have another 18 degrees of longitude to work with... -
Active mid December with multiple event potential
OSUmetstud replied to Typhoon Tip's topic in New England
Given the trailing trough catching up to the low thats awfully close to a big one here. -
You mean antibody test? Antigen test is for current infection.
-
Active mid December with multiple event potential
OSUmetstud replied to Typhoon Tip's topic in New England
Coastal Labrador. It's a beast 50/50 windstorm, not a snowstorm here. -
Active mid December with multiple event potential
OSUmetstud replied to Typhoon Tip's topic in New England
Rain and wind? -
Active mid December with multiple event potential
OSUmetstud replied to Typhoon Tip's topic in New England
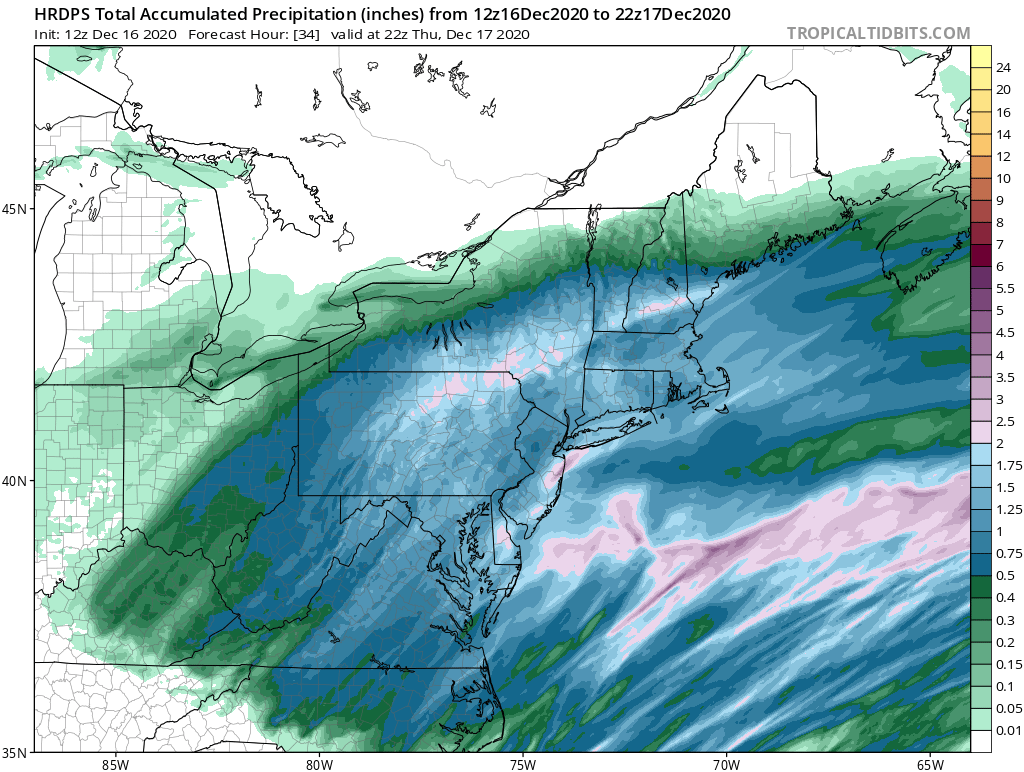
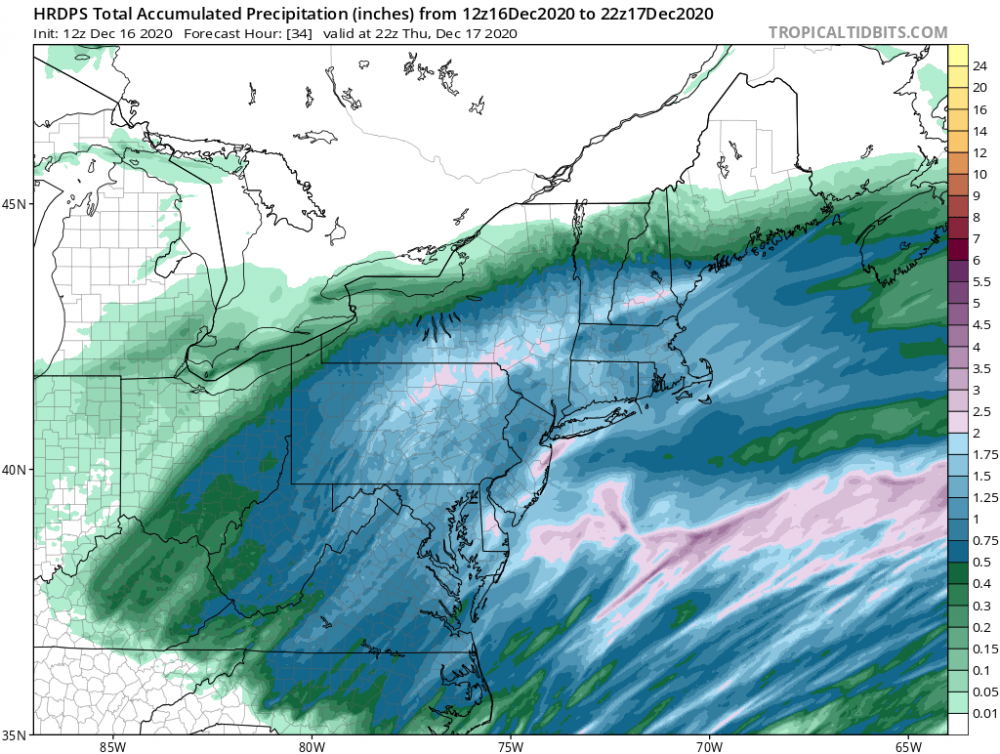
Idk, im hoping for further north solutions so that I get into some action Friday. Getting a SWFE now for 5 to 7 inches or so. -
Active mid December with multiple event potential
OSUmetstud replied to Typhoon Tip's topic in New England
It's a sad excuse for the 1950 Appalachian storm. -
Active mid December with multiple event potential
OSUmetstud replied to Typhoon Tip's topic in New England
Love the adiabatic cooling there over CT and MA. -
Active mid December with multiple event potential
OSUmetstud replied to Typhoon Tip's topic in New England
I'd toss the GFS... -
Active mid December with multiple event potential
OSUmetstud replied to Typhoon Tip's topic in New England
Im pretty sure that GFS run sets a pressure record for Newfoundland. It's like 937/938 over the Northern Peninsula. There's your 50/50 right there... -
Yes. Especially given he fought the virus through passive vaccination (the antibody therapy). Its possible he doesn't have his own antibodies and the injected one will wane and he won't have memory B cells. Fauci said he'd get the vaccine on camera...im hoping others will too.
-
Not a great look...though it sounded like it would have been done today or tomorrow anyway.
-
I'll be more confident that we hit peak when the positive rate starts to drop. As far as I've seen nationally speaking, it's still slowing going up.
-
I think this is the right interpretation...as in use some caution when making decisions based on the findings.
-
Richard can comment more on that but i thought it was 25%?
-
Its interesting data for sure. I'm guessing that all the restrictions in NY at the restaurants and gyms make them relatively safe (they wouldn't be under normal circumstances) whereas you cant do the same deal in the home.
-
Would it be really surprising to have a recession given the change in people's buying behaviors, government restrictions and the lack of stimulus?