ikcarsky
-
Posts
61 -
Joined
-
Last visited
Content Type
Profiles
Blogs
Forums
American Weather
Media Demo
Store
Gallery
Everything posted by ikcarsky
-
Masks mandates make many feel muzzled by the State. True. But that implies an even lower IFR, and even more immune individuals. In the end there's just no realistic scenario where surges in hospitalizations are maintained for long periods of time.
-
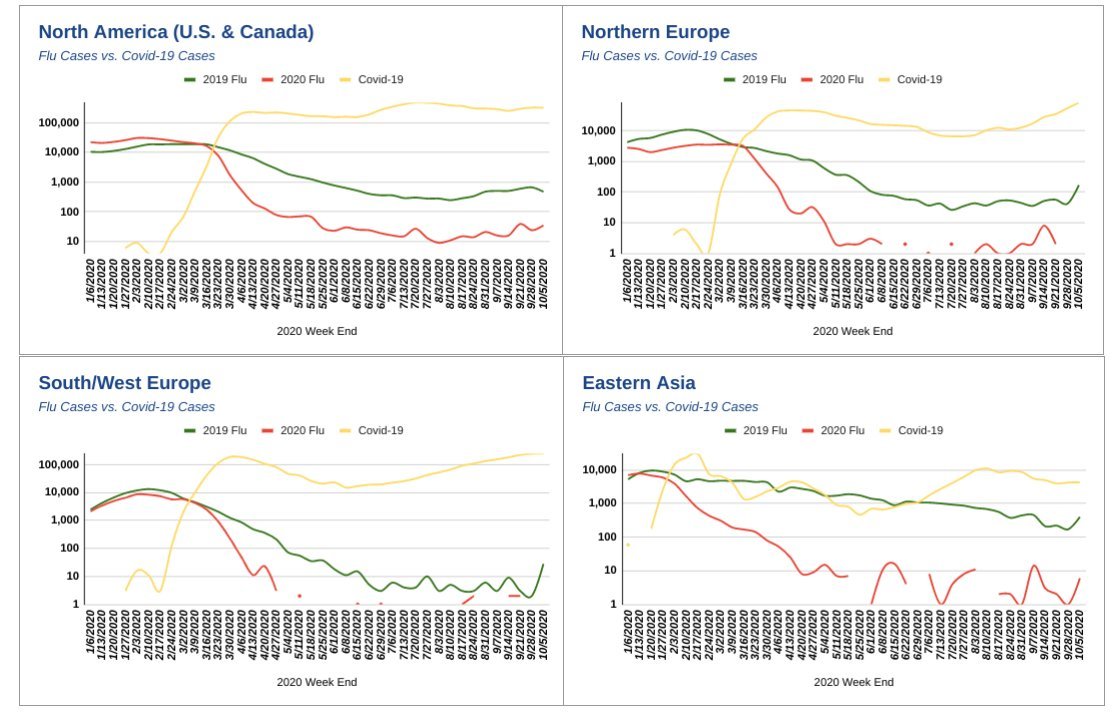
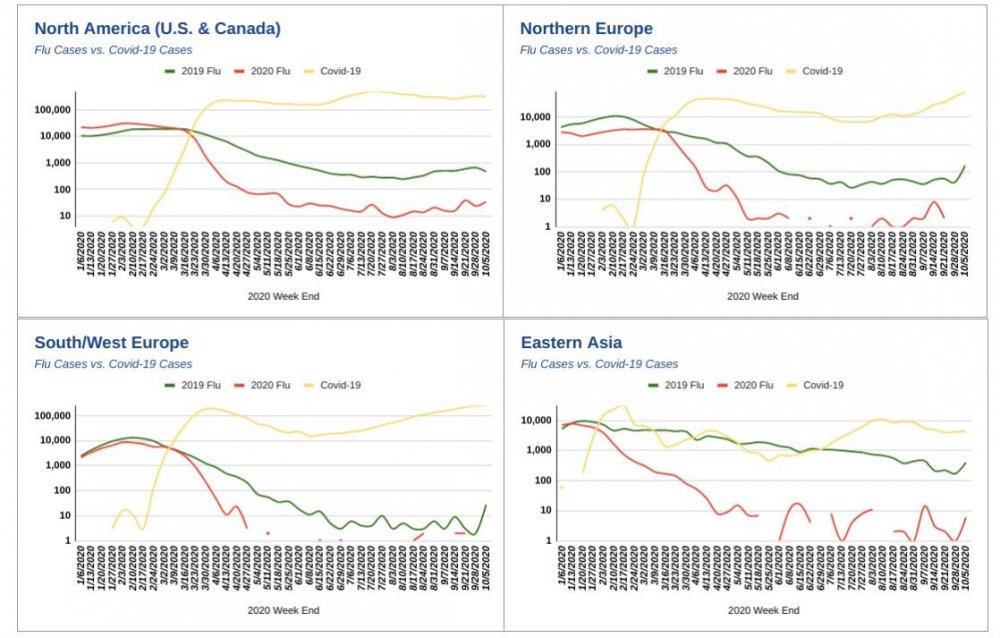
This is a gross exaggeration and unsupported by case and hospitalization data. Initial "first wave" case growth is exponential and hits the susceptible population hard when left unimpeded. Once the virus runs through this population and has to work through tougher, fitter organisms, the new infections generally lead to milder cases. We see this now in Europe where countries that crushed their first wave (Czech Republic) are seeing proportionally more severe cases than countries that were hit hard by their first wave (UK, France, etc.). Flu season is probably canceled, possibly because COVID is blocking it. Note how 2019 matched 2020 until COVID-19 popped up (log scale). And that's not for lack of flu testing either. We'll know for sure in a few weeks.
-
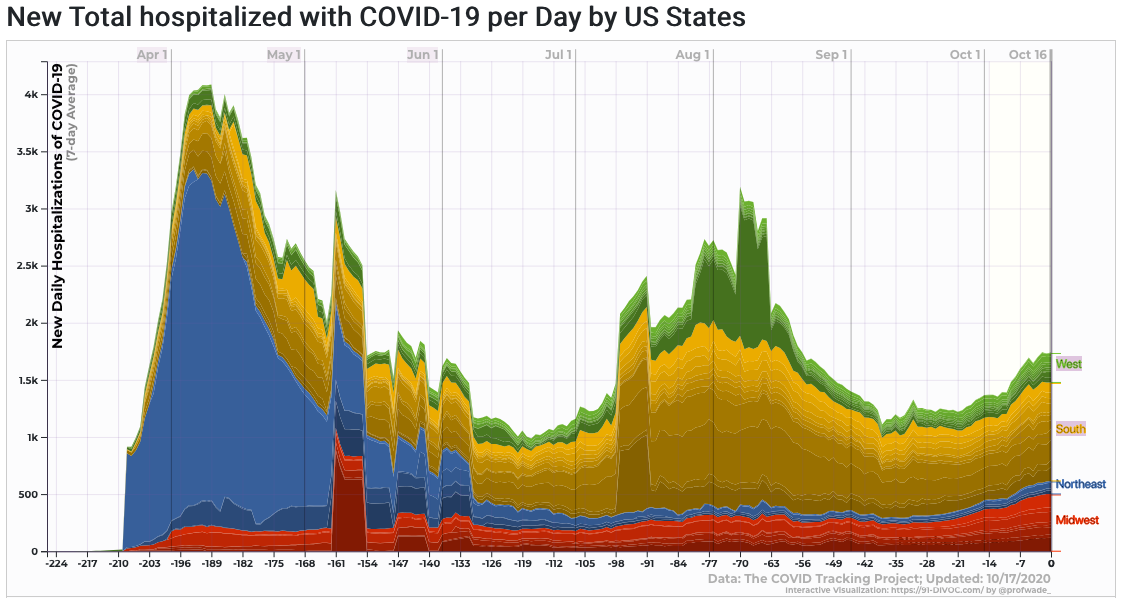
Data suggests this is a transient problem as the virus makes its first pass through the more susceptible population. This seems to be happening in states like WI now (and my state), where the spring surge was attenuated. But once the virus passes completely through the susceptible population the rate of hospitalizations drop. This may have happened in NYC, and I think that as autumn drags on we'll see their new cases go up while their hospitalizations will only rise slowly. Also we're getting better at treatment (those who remember my first rants in this thread know that I think we could be doing much better though). Still I do not disagree that making public health measures voluntary would be pretty rough for about 1% of the population. We know who they are mostly likely to be (elders with comorbidities), and they should voluntarily adopt their own protective measures.
-
At the risk of being "inhumane": it's time to accept defeat. The virus is now endemic, not just in the US but the West as a whole. It has won, and we've socially exhausted our ability to tolerate further lockdowns. We had our chance to make lockdowns work and we failed. Time to embrace that fact and restore overall quality of life by making all public health measures voluntary. If the State still wanted to do something useful, engage in mass distribution of Vitamin D and zinc supplements. Media messaging and narratives should change to encourage prophylaxis and overall fitness (e.g. outdoor activity, weight loss) should be emphasized. But ultimately let individuals take charge of their own health and act as they deem fit. And open up everything. (But I know this isn't going to happen.)
-
Nine months into this pandemic and there's still a lot we don't know. So many factors influence the spread of COVID-19, yet we all have a tendency to either wholly embrace or completely disregard the importance of any such factor depending on our biases. For example at this point I've heard it said that: Masks obviously don't work because of the new case surge (even though their ability to arrest droplets is beyond doubt) Masks work but the people are at fault for succumbing to lockdown fatigue (even though nearly all temperate NH states/countries are surging simultaneously) Cross-reactive T-cell immunity means herd immunity is almost here Cross-reactive T-cell immunity must be a myth (even though it is now well documented) The POTUS is to be blamed for the new surge in cases (in Europe too?) The POTUS can't be held responsible for any pandemic outcome (but is he not in charge?) I think there's at least a grain of truth in each one of these statements. But the question is how much? And how does this influence individual and authority action? Personally, I would let people take responsibility for their own health, and end all public health measures, save those which spread information about risk reduction. I understood the need for lockdown in the spring but now public health measures are really starting to take a severe social and economic toll, that in my estimation now outweigh the physical toll to be caused by the virus. But that's just in my biased estimation.
-
You are right; I should have been more careful. Still, the medicinal effects of CQ and HCQ are very similar (as are the molecules, a single hydroxy group makes the difference. Even the CDC page I linked lumps them together) and I at some point I began to assume equivalency in all respects. I looked into this a bit more and it appears HCQ is favored in modern times because the hydroxy group reduces the toxicity. Thanks for pointing that out. Having said that, the dosing in the UK RECOVERY trial (2.0 g in first 12 h, 0.4 g every 12 h for up to 9 days after that) still appears high to me. For acute malaria treatment, 1.6 g in first 24 h/2.0 g total in 48 h is standard; for prevention, the standard is merely 0.4 g per WEEK. Human toxicity studies are lacking (at least from what I could find) but if HCQ is really 2-3 times less toxic than CQ that puts a toxic dose of HCQ at around 3.0 g/24 h, thus the RECOVERY trial dosing is still cause for concern, especially given the long half-life of HCQ, many weeks. But it no longer seems maliciously bad. Good job. Not giving up on it though. Lots of publications now supporting my claim about the benefits of early administration. The first one linked therein, Ladapo et al., is a meta-analysis of five RCT studies. 24% reduction in cases found, p < 0.05, tells me HCQ works. And those studies were without regard to zinc, but I guess that's just magic to you.
-
Great, then maybe you can provide sources, I should like to read them. But the studies will have to be truly compelling, because now I have seen MANY studies that show a benefit to HCQ, especially when taken with zinc (as per the ionophore hypothesis), and given to patients early on in the progression of the disease. Obviously this is in complete opposition to your statement "no better than placebo".
-
Lol. Yes why should you believe me? All I did was demonstrate, using their own publication and other peer-reviewed literature, that the authors of the UK HCQ RECOVERY trial poisoned their HCQ arm using doses that even the CDC indirectly admits are so high that they're toxic. It's RIGHT THERE in my links, yet you refuse to look. It's okay, you don't need the blessing of a priest scientist to gaze upon the altar peer-reviewed literature. Though in your secular religion scientists are flawless and beyond reproach and I can tell I won't be able to convince you otherwise even when I thrust proof in your face. FWIW, I like the Covid crusher twitter because he doesn't link to articles by mainstream outlets, but directly to the scientific literature, often prior. There anyone can dig into the data, methodolgy, results, discussion, and conclusions, without any mainstream outlet to curate it for the masses. And when someone has their nose in the raw data, and the actual papers, they can bring valuable contributions not found elsewhere.
-
I linked directly to the CDC, the UK HCQ RECOVERY trial preprint, and the WHO. If that's QAnon trash I'm impressed; I wasn't aware he made reasoned arguments. Maybe I should take him more seriously? Meanwhile seasonality confirmed. The case trends in the NH are very synchronous, including in my state which is setting new case records.
-
And you know this for sure? Then maybe you can explain something to me. The CDC relies heavily upon the results of the UK HCQ RECOVERY trial in recommending against the use of HCQ. The CDC also just paragraphs later mentions 1.2 g in 24 h is a toxic dose of chloroquine (which is correct, and 2.0 g is often a lethal dose). So why I should I not discard the results of the UK RECOVERY investigation when they administered 2.4 g of HCQ in the first 24 h? And to gravely ill patients no less -- is that not absurd, when the hypothesized antiviral mechanism is inhibition of viral RNA replication, and should thus be studied principally in prophylaxis? Randomized and controlled means little when the study methodology is flawed. Or do you just know this because you this is what the mainstream media and their associated lab coat-wearing individuals told you to think, and if you question them you're a science denier?
-
So we can't act on reasonable hypotheses and mechanisms of action while we wait for the data to arrive? Hydroxychloroquine is one of our oldest drugs, closely related chloroquine is almost a century old. The scientific establishment has had plenty of time to realize these molecules have antiviral activity -- it has been suggested they help cells regulate their pH and take up zinc, thus inhibiting viral RNA replication. And because the side effect profile of HCQ is on par with aspirin, and the drug is dirt cheap, why not suggest it as a prophylactic? HCQ is already given prophylactically as an antimalarial. No need to go "but muh high power double blind placebo controlled trial" and sulk at home while waiting for that data to come. Same with Vitamin D and zinc. We know they are safe and help regulate immune function. Go supplement NOW. As to why the President stopped promotion of HCQ, well, remdesivir and Regeneron are IP controlled drugs -- unlike hydroxychloroquine. Thus very expensive, but very profitable for Gilead and Regeneron. I sense some incentives lined up here and the President was persuaded against HCQ. Or the doctors refused to administer it.
-
"Clearly"?